1.1 ACO Composition and Governance Structure
Tufts Health Public Plans, Inc. (THPP) and the Boston Children’s Health ACO, LLC (BCH ACO), have entered into an Accountable Care Partnership Plan (ACPP) Agreement with the shared aim of integrating behavioral and physical health and delivering high quality health care to improve the health of the pediatric MassHealth population.
The BCH ACO has entered into a management services agreement with Children’s Hospital Integrated Care Organization, LLC (CHICO), under which CHICO provides to the BCH ACO an executive management team, care management resources and operational support. Additionally, the BCH ACO engages CHICO to manage the ACO provider network that consists of Boston Children’s Hospital’s (BCH) primary care practices including Primary Care Longwood, the BCH Adolescent clinic and Martha Eliot primary care clinic; the Pediatric Physicians Organization, LLC (PPOC) participating primary care physicians; and the Physician’s Organization at Children’s Hospital, Inc. (PO), specialists employed by medical foundations affiliated with BCH (BCH Network).
Under the ACPP Agreement, THPP and the BCH ACO meet the structural requirements to operate as an MCO and an ACO, respectively. The governance structure and contractual arrangements contemplated by THPP and the BCH ACO to meet the Model A requirements, including the establishment of an ACPP Joint Operating Committee is shown in Figure 1 below.
Figure 1: THPP and BCH ACO Governing Structure
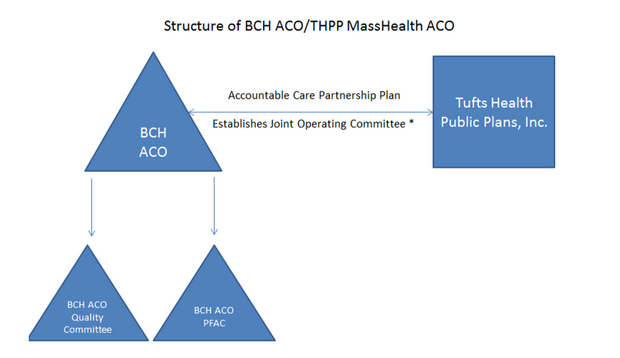
THPP and BCH ACO will leverage the Delivery System Reform Incentive Payment (DSRIP) opportunity to strengthen our collective ability to manage the attributed Medicaid population and the expected outcomes of improved quality and reduced total cost of care. The partners have agreed to allocate DSRIP funding, to the ACO partner, with the Joint Operating Committee overseeing decisions regarding annual DSRIP investment planning, conducting periodic progress review and managing reporting to EOHHS.
1.2 ACO Population Served
As of March 31, 2017, pursuant to the PY1 DSRIP Funding Notification Letter, BCH ACO has 83,403 attributed members. BCH ACO includes the following MassHealth service areas: Attleboro, Barnstable, Beverly, Boston, Brockton, Fall River, Falmouth, Framingham, Haverhill, Holyoke, Lawrence, Lowell, Lynn, Malden, New Bedford, Northampton, Orleans, Plymouth, Quincy, Revere, Salem, Somerville, Southbridge, Springfield, Taunton, Waltham, Wareham, Westfield, Woburn, and Worcester.
The majority of BCH ACO members receive primary care from a member provider of the PPOC. The PPOC is made up of more than 280 physicians in over 80 pediatric primary care practices in Eastern Massachusetts - from North of Boston to Metro West to Southeastern Massachusetts and Cape Cod. Primary care providers in the PPOC network offer members the care and convenience of a local community pediatrician with the addition of access to the BCH Network. The remaining BCH ACO members receive primary care delivered at the main campus of BCH and at Martha Eliot Health Center located in Boston’s Jamaica Plain neighborhood.
BCH has a long organizational history of understanding its populations and the communities in which they live. To better understand the needs of children, BCH conducts a comprehensive health needs assessment of local (Boston) priority neighborhoods (Dorchester, Fenway, Jamaica Plain, Mission Hill, and Roxbury) every three years. This assessment includes a review of public health data to examine health, social and economic indicators that affect a child’s health. The core of the assessment process is feedback from the community—youth, parents, neighborhood residents, other health providers, city leaders and many others—about what concerns them the most. The BCH community health needs assessment identified asthma, obesity, early childhood development, and special health care needs as key concerns for children and families in Boston Children’s priority neighborhoods. These conditions and concerns are also prevalent in other communities. An estimated 9% of the BCH ACO population has at least one chronic medical condition. Asthma is the most common chronic condition (over 4% of patients have asthma); rates are of particular concern in Boston and in communities in the South Coast region (over 5%). The PPOC has launched educational interventions aimed at improving the primary care management of patients with common conditions. In addition to asthma, to date, common conditions identified for this activity include headaches, gastroesophageal reflux, constipation, dermatologic conditions, ADHD, Down syndrome, and adolescent idiopathic scoliosis.
Limited access to mental health providers, particularly those who serve children and youth, has been identified as a key factor that contributes to high prevalence of undiagnosed or untreated conditions among both children and their parents. An estimated 14% of the BCH ACO population has a behavioral health condition. The BCH community health needs assessment identified behavioral health, including substance abuse, as a key health-related concern for children and families in BCH priority local (Boston) neighborhoods. The PPOC has identified numerous behavioral health needs among its patient population, including anxiety, depression, and eating disorders.
BCH is one of the lead organizations for the state’s Children’s Mental Health Campaign (CMHC), a coalition of families, advocates, health care providers, educators, and consumers from across Massachusetts dedicated to comprehensive reform of the children’s mental health system. Behavioral health needs that have been identified by the CMHC include psychiatric "boarding," when a child in mental health crisis requires inpatient psychiatric care, but there are no clinically appropriate resources, leading to prolonged stays in hospital Emergency Departments (EDs) or medical units; barriers that prevent children with mental and behavioral health problems from having a successful school experience; and unhealthy substance use by youth.
BCH estimates, based on the work of the Children’s Hospital Association nationally, that approximately 5-6% of all children in the BCH ACO population have complex medical needs, frequently impacting two or more body systems, and likely to result in serious lifetime impairments.
CHICO’s primary care network maintains specialized programs for children with very complex medical needs and uses a coordinated approach to the identification and care of children with developmental delays and chronic and congenital conditions. The Rainbow Program, based at BCH Primary Care at Longwood site, and a similar KASA program at Martha Eliot Health Center, coordinate integrated, multidisciplinary care for approximately 1,000 children with complex medical needs, most of whom are covered by MassHealth.
BCH community health needs assessment identified poverty, education, access to affordable housing, neighborhood safety, and food security as key individual and community concerns. For example, the number of homeless individuals in Boston steadily increased between 2009 and 2013, and there was a 25% increase in the reported numbers of homeless families between 2013 and 2015. BCH -based primary care practices focus on care for children living in poverty, and the PPOC serves many families with social needs that contribute to uncontrolled illness and affect the family’s ability to keep the child healthy.
In addition to the salient health and health-related social characteristics of the population noted in other areas of this Section, our needs assessment and other evaluation activities have identified early childhood education and health services as key for this population of pediatric patients. Concerns for this critical developmental stage include gaps in access to screening, early intervention and early education services, and additional programs that support the parents of young children in identifying delays and promoting healthy child development. BCH community needs assessments have traditionally focused on the local neighborhoods surrounding BCH. BCH ACO and THPP anticipate identifying and serving similar needs across the state.
1.3 Overview of DSRIP Investment Approach
BCH ACO has taken a deliberately ‘conservative’ approach to ‘valuing’ DSRIP investment; rolling over funds to the extent permissible and deploying existing resources differently in many ways across the enterprise in the first years of the contract.
In PY0 and PY1, BCH ACO will utilize DSRIP funding to realign existing resources with ACO requirements. In PY1 and PY2, BCH ACO will make small-scale pilot investments with limited net new spending. In PY3 and PY4, the ACO will scale validated programs. In PY5 and beyond, anticipated program costs will be offset with demonstrated savings.
The success of the ACO depends on the improvement of care, the measurable improvement of quality, and the reduction of total medical expense for this population. Complete annual data on BCH ACO population expenditures will not be available until PY2 and we expect that we will gather credible information on where the best investments and sustainability lie by PY3.
The overall clinical direction of the ACO focuses on three primary areas: 1) care of children with complex needs; 2) expansion and access to behavioral health services; and 3) the assessment of social determinants of health and outreach for prevention and wellness. Specific initiatives for each of these clinical areas will be established with measurable outcomes and a plan for delivery of services. Other clinical opportunities that will be addressed to reduce the overall cost of care include the reduction of specialty visits and better coordinated specialty care, and analytics and programming to better identify patients and families over-utilizing acute care for low acuity patient needs. BCH ACO anticipates that DSRIP funding in Years 1 and 2 will augment the work begun in Year 0, including continuing or supplementing previously-grant funded programs, as well as launching certain new programs. Funding from DSRIP will support programs across the continuum of care through Year 3, after which we anticipate the need for support funding to wind down, as we narrow down to programs with demonstrated sustainability with renewable funding sources.
Each clinical initiative will have a TME target, which will be established with analytics during the initial phase of the program and continuously refined. The initiatives will combine care improvement and care coordination as well as measurement of elements of utilization (e.g., hospital days, ED visits or pharmacy unit cost) that impact TME so that we can understand the investment return when new staffing or other resources are required for ongoing implementation. The intent is that services funded by DSRIP will be sustainable by the reduction of total medical spending, which may include increasing certain billable services (e.g., behavioral health treatment) while improving overall TME. There are some infrastructure areas (for example, analytics) that do not have direct return on investment and cost savings so these will be attributed as ongoing expenses. It will take until 2020 to identify which initiatives are independently sustainable.
There are a number of inherent risks to the program. This population of patients can have unique social and medical challenges. Historically patient care has not been managed using an accountable care approach and the cultural shifts for clinicians, practices and patients are significant. The data integrity to support this work is evolving as well. Together, this leaves a great deal of uncertainty with regard to the adequacy of rates and administrative expenses that are funded through the global budget as well as DSRIP.
1.4 Website
Print version
Boston Children's Accountable Care Organization in partnership with Tufts Health Public Plans (English, PDF 142.19 KB)