Section 1: Employee applying for family leave to care for a family member
The employee who is applying for paid family leave to care for your patient should complete Section 1 of the Certification of Your Family Member's Serious Health Condition form.
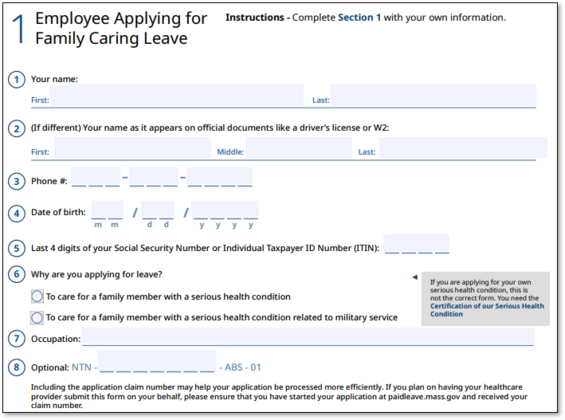
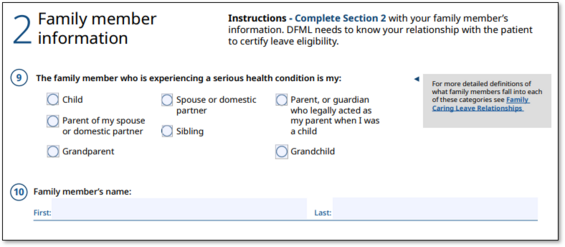
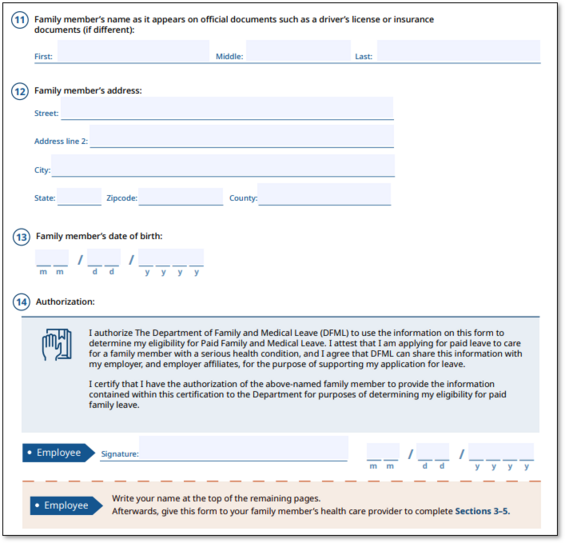
Section 2: Family member information
The employee should enter information about their family member, your patient, to complete Section 2.
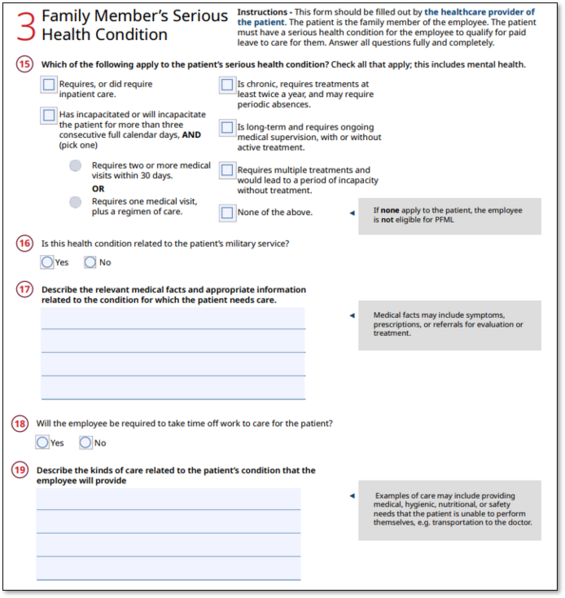
Section 3: Family member's serious health condition
You, as the health care provider, should complete Section 3 through Section 5.
In Section 3, confirm that your patient has a serious health condition and what criteria apply.
- Confirm if it is related to the patient's military service.
- Note any relevant medical information about your patient that shows that they will require care.
- Describe the kinds of care your patient might need.
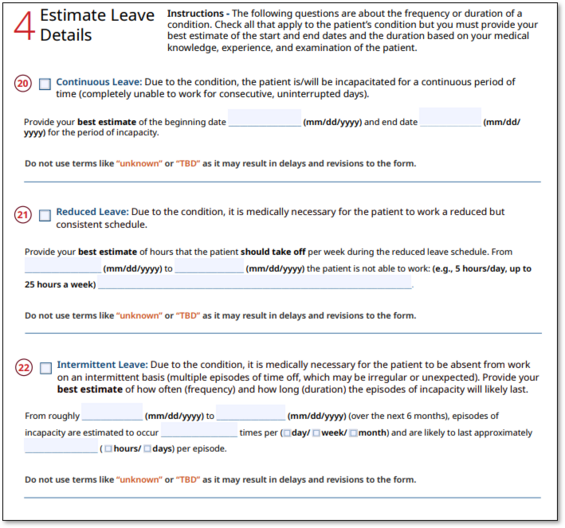
Section 4: Estimate leave details
Provide your best estimate on what type of leave schedule will be needed: continuous, reduced, intermittent, or a combination of the three.
- Continuous leave: Full-time leave taken without interruptions
- Reduced leave: Consistent schedule that is less than an employee's regular work schedule
- Intermittent leave: Leave taken in separate periods of time due to a single qualifying reason
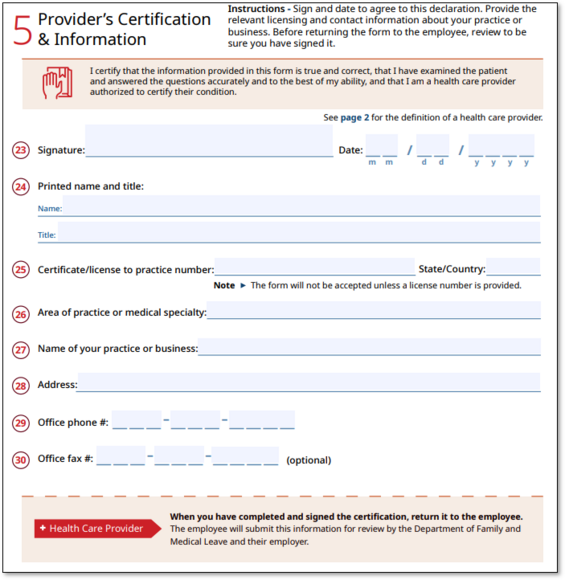
Section 5: Provider's certification and information
Provide information on your certification, and area of practice or medical specialty.
Review the form and make sure you have signed it before returning it to the employee.
Contact
Phone
Department of Family and Medical Leave - Hours of operation: Monday-Friday, 8 a.m. - 4:30 p.m.
Department of Family and Medical Leave - Hours of operation: Monday-Friday, 8 a.m. - 4:30 p.m.
Department of Revenue - Hours of operation: Monday-Friday, 8:30 a.m. - 4:30 p.m.
| Last updated: | August 22, 2025 |
|---|