Primary Stroke Service Overview
Primary Stroke Service (PSS) designation in Massachusetts indicates that a health care facility is ready to evaluate and treat acute stroke patients 24 hours a day. Massachusetts PSS facilities submit data to the Bureau of Health Care Safety and Quality (BHCSQ) as part of licensing.
Stroke treatment
After clinical evaluation by a doctor, eligible patients with acute ischemic strokes (strokes that are caused by a blood clot that blocks a blood vessel in the brain and prevents blood from flowing to the brain) can be treated with alteplase, a drug that dissolves stroke causing clots, to improve patient recovery and outcome. Evaluation for treatment involves ruling out medical contraindications, or reasons that a particular drug should not be used, and assessment by computerized tomography (CT).
Current recommendations encourage prompt evaluation and treatment of eligible patients, specifically that facilities should perform a CT scan and administer alteplase treatment within 60 minutes of when a patient arrives at a facility. Research also shows that treatment can be effective in an expanded window of 4.5 hours, from the time that the patient is last known to be well (last known well or “LKW”) to the time treatment is provided.
Findings from Massachusetts PSS Facilities
Massachusetts PSS Facility Reported Stroke Characteristics, 2018 (N=15,390)
| Stroke Type | Count | Percent |
|---|---|---|
| Ischemic | 10,436 | 67.8 |
| Transient Ischemic | 2,585 | 16.8 |
| Subarachniod | 598 | 3.9 |
| Hemorrhagic | 1,730 | 11.2 |
| Not otherwise specified | 41 | 0.27 |
| Race | Count | Percent |
|---|---|---|
| White | 12,729 | 82.7 |
| Black and African American | 1,219 | 7.9 |
| Asian | 462 | 3.0 |
| American Indian/Alaska Native | 28 | 0.2 |
| Hawaiian/Pacific Islander | 9 | 0.1 |
| Multi and other | 15 | 0.1 |
| Undetermined | 928 | 6.0 |
| Hispanic Ethnicity | 780 | 5.1 |
| Gender | Count | Percent |
|---|---|---|
| Female | 7,880 | 51.2 |
- In 2018, 68 Massachusetts PSS facilities reported 15,390 strokes*, including 10,436 ischemic strokes (67.8%). If ischemic strokes are identified quickly, they can be treated with alteplase.
- Among stroke patients, the median age was 74 years and the mean age was 72 years.
- National Institute of Health Stroke Scale/Score (NIHSS) measures the severity of a stroke on a scale of 0 to 42, with a lower score representing a lower severity stroke. In 2018, the MA median score among reported patients was 3.
- 7,880 (51%) of all reported strokes occurred in women.
- 928 patients (6.0%) had no race data submitted, which may result in undercounting of some groups.
- 780 (5.1%) strokes were reported in patients of Hispanic ethnicity.
- The median time from arrival at the facility to CT scan was 24 minutes among ischemic stroke patients.
- Among ischemic stroke patients treated with alteplase, the median time from last known well to treatment was 135 minutes.
*Please note that this does not include patients who had elective carotid procedures, no stroke related diagnosis, or had symptom onset while already admitted to an acute care facility
Patient transport to stroke hospitals
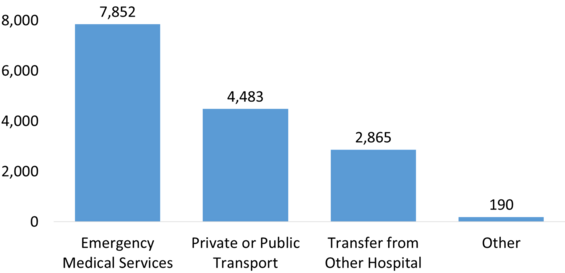
Patients arriving by Emergency Medical Services (ambulance) have better outcomes and numerous stroke awareness campaigns advocate calling 911.
- For ischemic strokes, the median time from LKW to emergency department arrival was 4.8 hours**
- 4,483 patients (29%) arrive at the emergency department in a private vehicle or on public transportation, which may delay facility arrival
**Does not include patients who left against medical advice or died during stroke admission
Patients with ischemic stroke and documented last known well time
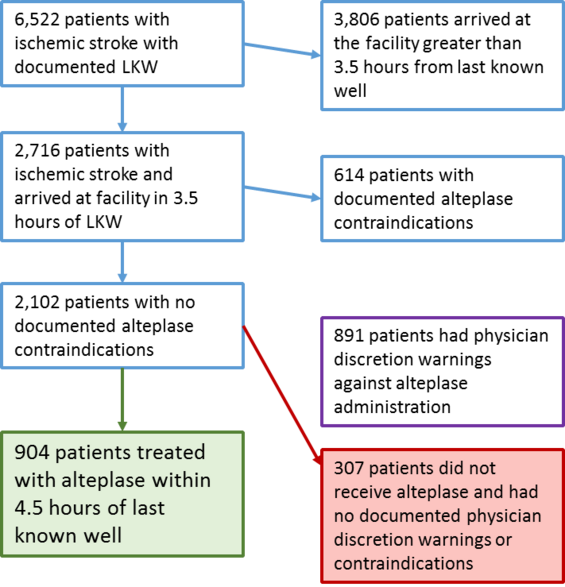
- 6,522 had time of last known well (LKW) documented, but only 2,716 of these arrived at a PSS facility within 3.5 hours. This arrival window allows enough time for a patient to be evaluated and treated with alteplase, if appropriate.
- 614 patients had contraindications and were not treated, and an additional 891 patients had documented physician discretion warnings.
- 904 (43%) of ischemic stroke patients who arrived in 3.5 hours and had no drug contraindications were treated with alteplase within 4.5 hours.
- 307 (14.6%) of these patients were not treated with alteplase and had no documented physician discretion warnings.
- 335 patients arriving within 3.5 hours of LKW did not have a CT performed within 60 minutes of ED arrival.
“Top 5 Physician Discretion Warnings:”
- Rapid improvement
- Severity too mild
- Patient or family refusal
- Facility unable to determine eligibility
- Seizure at onset with postictal residual neurological impairment
Recommendations
- Not all patients that could benefit from alteplase are receiving treatment in the expanded 4.5 hour window. Outside of label contraindications, the most common reported reasons for not administering alteplase are the stroke severity is too mild or refusal by the patient or family. Additional education and provider communication with patients and their families could reduce treatment refusal.
- 29% of reported strokes arrived at the hospital in a private vehicle or on public transportation. Many public awareness campaigns, including FAST advocate calling 9-1-1. Additional education, at the community and facility level, is needed to encourage EMS use.
Methodology & sources
Methods
Data were extracted from the MA PSS module on August 14, 2019, only completed patients discharged between January 1, 2018 and December 31, 2018 were included. All patients already admitted to an acute care facility or admitted for elective carotid procedures or no stroke diagnosis were excluded. Patient evaluation and treatment for alteplase treatment was limited to completed patients records diagnosed with ischemic stroke with a documented last known well date and time. Acute length of stay calculation excludes patient who left against medical advice, died, or were transferred to another acute care facility.
Sources
- Wardlaw JM, et al. Recombinant tissue plasminogen activator for acute ischemic stroke. Lancet. 2012;370(9834):2364-2372.
- Jauch, E.C., Saver, J.L., et al. (2013). Guidelines for the Early Management of patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke, 44 (3), 870-947.
- Hacke, W., Kaste, M., et al. (2008). Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke. The New England Journal of Medicine, 359, 1317-1329.
- United Kingdom Department of Health (2009, Feb 9). Stroke: Act F.A.S.T. Awareness Campaign. Retrieved from the United Kingdom National Archives (2019, Oct 2).
Additional Resources
-
Open PDF file, 523.54 KB, Massachusetts Primary Stroke Service Data Brief (English, PDF 523.54 KB)